Are Doctors Choosing Wisely Yet?
The ABIM Foundation’s initiative to cut healthcare waste has compiled hundreds of suggestions. Getting doctors on board will be a different story.


In 2012, the American Board of Internal Medicine (ABIM) Foundation launched Choosing Wisely, an educational program aimed at encouraging physicians to steer clear of low-value and wasteful procedures and tests. The initiative works on a hub-and-spoke model, positioned at the center of a growing number of specialty societies that disseminate its recommendations to their physician members.
If Choosing Wisely achieved its mission in full, “We’d reduce overutilization significantly, have better quality, harm [fewer] people unnecessarily, and—as a byproduct—we’d be saving close to $200 billion a year,” ABIM Foundation Executive Vice President and COO Daniel Wolfson told Healthcare Analytics News™ (HCA News) when asked what healthcare would look like.
But the program looks as if it has a long way to go before that. In late 2017, Health Affairs published 2 reports on the campaign’s impact to date and its outlook. The retrospective report looked at 2 surveys (one from 2014 and another from 2017) to evaluate whether physicians’ views of low-value services and the Choosing Wisely program had changed since its launch.
>>Read: CMS is Leading the Way Toward Bundled Payments. Should It Be?
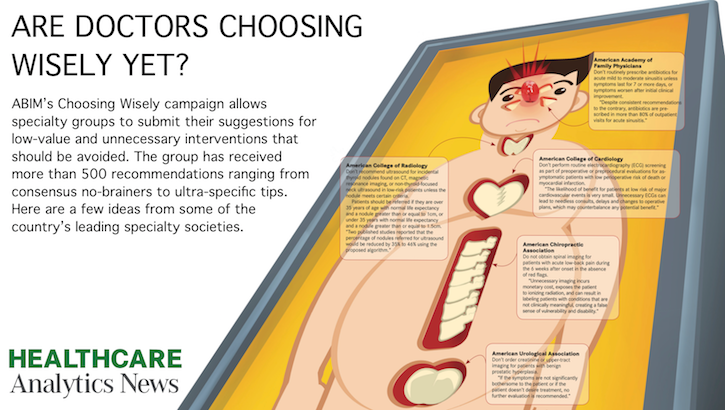
There were about a dozen slam-dunk procedures that investigators chose to ask doctors about in the study: “Don’t do imaging for low back pain when no red flags are present. Don’t order upper tract imaging for patients with benign prostatic hyperplasia. Don’t order cardiac tests on low-risk, asymptomatic patients. Don’t screen women older than 65 for cervical cancer who have had prior screening and are not otherwise at high risk for it,” were among the points listed by author Alexander Mainor, MPH, of the Dartmouth Institute for Health Policy and Clinical Practice.
And there was some improvement. In 2017, 46% of physicians, without having been prompted, reported having had conversations about the value of those procedures with patients, compared with 42% surveyed in 2014.
A quarter of physicians polled in 2017 acknowledged that they were familiar with the campaign. That number climbed slightly from 21% in 2014. After physicians received a description of the initiative, that number came to about 4 in 10 for both years (39% in 2014 and 42% in 2017). In both surveys, primary care physicians were significantly more likely than specialists to be aware of the efforts.
“We were a bit surprised that we didn’t see significant increases in awareness of the campaign at first, but we place it in the broader context of how difficult it is to try to disseminate innovation in healthcare systems,” Mainor told HCA News. “It takes an average of 17 years for new information to actually reach clinical practice. Along that timeline, the Choosing Wisely campaign really isn’t that old.”
His report noted that previous surveys found that some of the program’s recommendations had been “difficult for physicians to follow and for patients to accept.” Overwhelmingly, physicians felt “very comfortable” talking to patients about why they should avoid low-value procedures, but that number actually fell from 82% to 74% from 2014 to 2017. A higher percentage indicated that it had become harder in the preceding years for them to have such conversations.
Overall, the leading reasons physicians gave for ordering tests and procedures that may have been unnecessary were malpractice concerns (87%), desire to reduce uncertainty (84%), and “just to be safe” (78%). Mainor and his coauthor and Dartmouth colleague, Carrie Colla, PhD, noted that such so-called defensive medicine has been found in studies to account for as much as 3% of American healthcare spending.
But Wolfson said defensive medicine is more of a scapegoat, noting that things like malpractice concerns “minimize other reasons” why physicians may be slow to eliminate low-value procedures. Many of them, he said, are systemic and cultural.
“It’s a complex problem. I think the number one reason is thoroughness, the way they’re trained,” he said. “Physicians are trained to be thorough, leave no rock unturned. There’s also fee-for-service, the volume driver.”
Education is another huge part of the equation. Many physicians passed through medical school long before value-based care had entered the healthcare consciousness. Value-centric conversations between physicians and patients simply weren’t taking place even a few years ago, Mainor said.
The success that the program has had so far, he and Wolfson said, was in recruiting specialty societies and compiling a large list of tests and procedures that may qualify as low value. In its first year, the program enlisted 9 societies; in the next year, it added 17 more. Today, more than 80 participate.
Wolfson said the model gives Choosing Wisely great reach and also gives physicians a say in which interventions the campaign may choose to focus on. The group has had more than 500 different test and procedure cases suggested for their consideration.
Those suggestions are all listed on the campaign’s website, sorted by area of medicine. They range from the American Academy of Nursing’s insistence on skin-to-skin contact between mother and child immediately after birth to the sort of near-consensus value recommendations that Mainor and Colla asked physicians about in their study.
But the tricky thing is turning those hundreds of new recommendations into real, value-based change instead of more information that physicians are expected to remember. Wolfson recommended building the suggestions into clinical decision support and ordering tools within the electronic medical records system to get them before doctors’ eyes at the point of care.
The coinciding forward-looking report championed the program’s rapid growth, but it has 3 suggestions of its own. The first is that societies be given incentive to work together to codify and consolidate recommendations. The other 2 have to do with validating suggestions, first by adjusting for “multiphasic drivers of overuse of services” and second by engaging stakeholders beyond specialty societies—patients, health systems, and the “volume drivers” that Wolfson referred to, insurance companies—to actually test the economics of avoiding certain services. Studies will need to be more sophisticated in order to be accurate, and it will take time to complete them.
That report is still optimistic about Choosing Wisely’s future. Wolfson, however, is even more so. “We need to continue to work on awareness, and now we’re focused on how other organizations think about local delivery systems,” he said. “Massive change takes 15 years. We’re dedicated to doing it sooner, 10 years, but we feel like this has just begun.”
Related Coverage:
Hunting for the Heart of a Changing Community
CMS is Leading the Way Toward Bundled Payments. Should It Be?
Precision Medicine, Sure. But What About Precision Payments?











Children’s hospitals face complex challenges dealing with disasters
April 18th 2025Pediatric hospitals deal with different factors in weather-related events and other emergencies. Terri Wilson of the Children’s Hospital Association talks about the challenges and the need for more planning and support.



Telehealth faces a looming deadline in Washington | Healthy Bottom Line podcast
February 12th 2025Once again, the clock is ticking on waivers for telemedicine and hospital-at-home programs. Kyle Zebley of the American Telemedicine Association talks about the push on Congress and the White House.



